Printable DD 2870 Template
The DD 2870 form is an essential document used within the Department of Defense, particularly for those seeking to request a waiver or exemption related to certain military benefits. This form serves as a formal request for information and is critical for service members and their families navigating the complexities of military benefits and entitlements. Completing the DD 2870 accurately is vital, as it can significantly impact eligibility for various programs, including healthcare and education benefits. The form requires detailed information about the applicant, including personal identification details and the specific benefits being requested. Understanding the requirements and implications of the DD 2870 is crucial for ensuring that service members receive the support they deserve. Properly filling out this form can facilitate a smoother process in obtaining necessary waivers, making it an important step in managing military-related benefits.
Common mistakes
-
Incomplete Information: One common mistake is failing to fill out all required fields. Every section must be addressed to ensure the form is processed without delays.
-
Incorrect Personal Information: Individuals sometimes enter incorrect names, Social Security numbers, or dates of birth. Double-checking this information is crucial for accurate identification.
-
Missing Signatures: Forgetting to sign the form is a frequent oversight. A signature is necessary to validate the information provided and to confirm consent.
-
Failure to Provide Supporting Documentation: Some people neglect to include required documents, such as proof of eligibility. This can lead to delays in processing the request.
-
Using Incorrect Form Version: It's important to ensure that the most current version of the DD 2870 is used. Outdated forms may not be accepted.
-
Not Following Submission Guidelines: Each submission may have specific instructions regarding how to send the form. Ignoring these can result in complications.
-
Overlooking Deadlines: Individuals may miss important deadlines for submitting the form. Keeping track of timelines is essential to avoid any interruptions in benefits.
-
Assuming Help is Not Available: Some people hesitate to seek assistance when filling out the form. Resources and support are often available, and asking for help can prevent mistakes.
Find Common Documents
Simple Owner Operator Lease Agreement - Any exemptions from liability or limitations in Owner Operator’s documents are rendered ineffective unless explicitly stated.
In addition to the essential management structure and operational procedures outlined in the California Operating Agreement form, it is advisable to refer to resources like California Templates to ensure all necessary details are accurately captured for effective LLC operation.
Act of Donation of a Movable Louisiana - This form ensures that the donation is properly documented and recognized under Louisiana law.
I-589 Application - Filing the I-589 comes with a need for careful attention to each question's requirements.
Key takeaways
Filling out the DD 2870 form is an important process for individuals seeking to access their medical records or other health-related information. Here are some key takeaways to keep in mind:
- Understand the Purpose: The DD 2870 form is used to authorize the release of medical information. Knowing this helps clarify why you need the form.
- Complete All Sections: Ensure that every section of the form is filled out completely. Incomplete forms may lead to delays.
- Provide Accurate Information: Double-check all personal information, including your name, address, and contact details. Accuracy is crucial.
- Signature Requirement: Your signature is necessary on the form to validate the request. Make sure it is legible.
- Specify the Information Needed: Clearly indicate what specific records you are requesting. This helps the provider fulfill your request promptly.
- Understand the Privacy Implications: By signing the form, you are allowing access to your personal health information. Be aware of who will receive this information.
- Check Submission Guidelines: Different facilities may have different procedures for submitting the form. Be sure to follow the specific guidelines provided.
- Keep a Copy: After submitting the form, retain a copy for your records. This can be useful for future reference.
- Follow Up: If you do not receive a response within a reasonable time, consider following up to ensure your request is being processed.
- Seek Assistance if Needed: If you have questions or need help, do not hesitate to reach out to the appropriate office or a trusted advisor.
By keeping these key points in mind, you can navigate the process of using the DD 2870 form more effectively and with greater confidence.
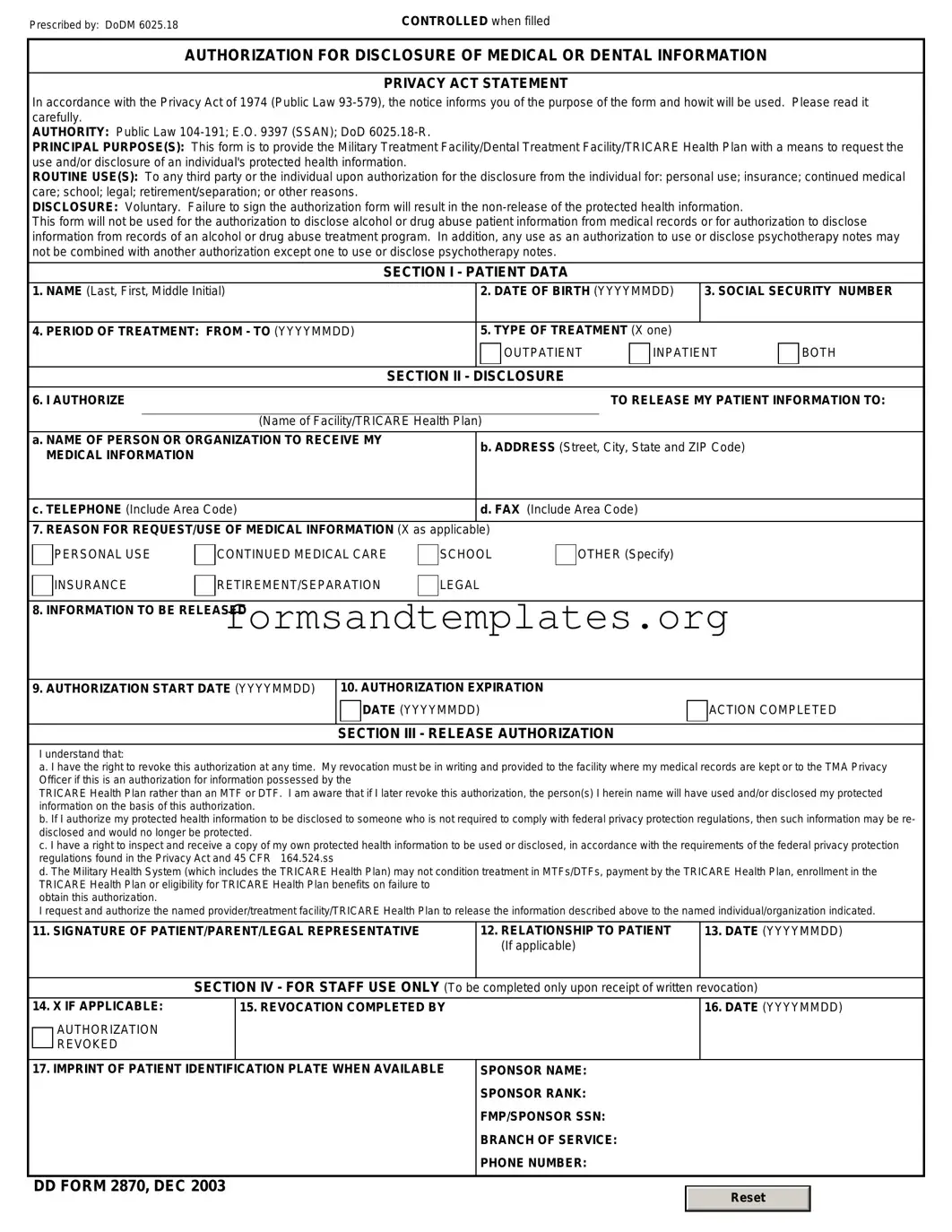
DD 2870 Example
Prescribed by: DoDM 6025.18 |
CONTROLLED when filled |
AUTHORIZATION FOR DISCLOSURE OF MEDICAL OR DENTAL INFORMATION
PRIVACY ACT STATEMENT
In accordance with the Privacy Act of 1974 (Public Law
AUTHORITY: Public Law
PRINCIPAL PURPOSE(S): This form is to provide the Military Treatment Facility/Dental Treatment Facility/TRICARE Health Plan with a means to request the use and/or disclosure of an individual's protected health information.
ROUTINE USE(S): To any third party or the individual upon authorization for the disclosure from the individual for: personal use; insurance; continued medical care; school; legal; retirement/separation; or other reasons.
DISCLOSURE: Voluntary. Failure to sign the authorization form will result in the
This form will not be used for the authorization to disclose alcohol or drug abuse patient information from medical records or for authorization to disclose information from records of an alcohol or drug abuse treatment program. In addition, any use as an authorization to use or disclose psychotherapy notes may not be combined with another authorization except one to use or disclose psychotherapy notes.
SECTION I - PATIENT DATA
1. NAME (Last, First, Middle Initial) |
|
2. DATE OF BIRTH (YYYYMMDD) |
3. SOCIAL SECURITY NUMBER |
|||
|
|
|
|
|
|
|
4. PERIOD OF TREATMENT: FROM - TO (YYYYMMDD) |
|
5. TYPE OF TREATMENT (X one) |
|
|
||
|
|
|
OUTPATIENT |
INPATIENT |
BOTH |
|
|
|
|
|
|
|
|
|
|
SECTION II - |
DISCLOSURE |
|
|
|
6. I AUTHORIZE |
|
|
TO RELEASE MY PATIENT INFORMATION TO: |
|||
|
|
|
|
|
||
|
(Name of Facility/TRICARE Health Plan) |
|
|
|
||
a. NAME OF PERSON OR ORGANIZATION TO RECEIVE MY |
|
b. ADDRESS (Street, City, State and ZIP Code) |
|
|||
MEDICAL INFORMATION |
|
|
||||
|
|
|
|
|
||
|
|
|
|
|
||
c. TELEPHONE (Include Area Code) |
|
d. FAX (Include Area Code) |
|
|
||
|
|
|
|
|
||
7. REASON FOR REQUEST/USE OF MEDICAL INFORMATION (X as applicable) |
|
|
|
|
||
PERSONAL USE
INSURANCE
CONTINUED MEDICAL CARE
RETIREMENT/SEPARATION
SCHOOL
LEGAL
OTHER (Specify)
8. INFORMATION TO BE RELEASED
9. AUTHORIZATION START DATE (YYYYMMDD)
10. AUTHORIZATION EXPIRATION
DATE (YYYYMMDD)
SECTION III - RELEASE AUTHORIZATION
ACTION COMPLETED
I understand that:
a. I have the right to revoke this authorization at any time. My revocation must be in writing and provided to the facility where my medical records are kept or to the TMA Privacy Officer if this is an authorization for information possessed by the
TRICARE Health Plan rather than an MTF or DTF. I am aware that if I later revoke this authorization, the person(s) I herein name will have used and/or disclosed my protected information on the basis of this authorization.
b. If I authorize my protected health information to be disclosed to someone who is not required to comply with federal privacy protection regulations, then such information may be re- disclosed and would no longer be protected.
c. I have a right to inspect and receive a copy of my own protected health information to be used or disclosed, in accordance with the requirements of the federal privacy protection regulations found in the Privacy Act and 45 CFR 164.524.ss
d. The Military Health System (which includes the TRICARE Health Plan) may not condition treatment in MTFs/DTFs, payment by the TRICARE Health Plan, enrollment in the TRICARE Health Plan or eligibility for TRICARE Health Plan benefits on failure to
obtain this authorization.
I request and authorize the named provider/treatment facility/TRICARE Health Plan to release the information described above to the named individual/organization indicated.
11. SIGNATURE OF PATIENT/PARENT/LEGAL REPRESENTATIVE |
12. RELATIONSHIP TO PATIENT |
13. DATE (YYYYMMDD) |
|
(If applicable) |
|
|
|
|
SECTION IV - FOR STAFF USE ONLY (To be |
completed only upon receipt of written revocation) |
|
14. X IF APPLICABLE:
AUTHORIZATION REVOKED
15. REVOCATION COMPLETED BY
16.DATE (YYYYMMDD)
17. IMPRINT OF PATIENT IDENTIFICATION PLATE WHEN AVAILABLE |
SPONSOR NAME: |
||
|
SPONSOR RANK: |
||
|
FMP/SPONSOR SSN: |
||
|
BRANCH OF SERVICE: |
||
|
PHONE NUMBER: |
||
|
|
|
|
DD FORM 2870, DEC 2003 |
|
|
|
|
Reset |
|
|
|
|
|
|
|
|
|
|
Understanding DD 2870
- Your personal details, including name, rank, and contact information.
- The name and contact information of the person or organization you are authorizing to receive your information.
- A description of the information you wish to disclose.
- The purpose for which the information will be used.
- Your signature and date to confirm your authorization.
What is the DD 2870 form?
The DD 2870 form, also known as the "Authorization for Disclosure of Medical or Dental Information," is a document used by the Department of Defense. It allows service members and their dependents to authorize the release of medical or dental information to specific individuals or organizations. This form ensures that sensitive health information is shared only with those who have permission to receive it.
Who needs to fill out the DD 2870 form?
Any service member or dependent who wants to allow someone else to access their medical or dental records should fill out the DD 2870 form. This could include parents, spouses, or other family members who may need information for various reasons, such as coordinating care or handling medical bills.
How do I obtain the DD 2870 form?
The DD 2870 form can be obtained from various sources. You can find it on the official Department of Defense website, or you may request it from your healthcare provider's office. Additionally, military medical facilities often have copies available for patients.
What information do I need to provide on the form?
When filling out the DD 2870 form, you will need to provide the following information:
How long is the DD 2870 form valid?
The DD 2870 form does not have a specific expiration date. However, it is generally advisable to renew the authorization periodically, especially if there are changes in your medical situation or the individuals authorized to receive your information. This ensures that your preferences remain current and respected.
Can I revoke my authorization after submitting the DD 2870 form?
Yes, you can revoke your authorization at any time. To do this, you should submit a written request to the healthcare provider or organization that received the original DD 2870 form. This request should clearly state that you wish to revoke your authorization, and it is helpful to include your personal information for identification purposes.
What happens if I do not fill out the DD 2870 form?
If you do not fill out the DD 2870 form, your medical or dental information will remain confidential and will not be shared with anyone else. This means that if you need someone to help manage your healthcare or handle medical bills, they will not have access to your records without your explicit permission.
Where should I submit the completed DD 2870 form?
Once you have completed the DD 2870 form, you should submit it to the appropriate healthcare provider or organization. This could be a military medical facility, a civilian healthcare provider, or any other entity that requires access to your medical or dental information. Make sure to keep a copy for your records.
Is there a fee associated with using the DD 2870 form?
Typically, there is no fee for filling out or submitting the DD 2870 form itself. However, some healthcare providers may charge a fee for copying or processing medical records. It is advisable to check with the specific provider regarding any potential costs associated with obtaining your records.
How to Use DD 2870
After obtaining the DD 2870 form, it's important to ensure that all necessary information is accurately filled out. This process will help in facilitating the next steps in your request. Follow the steps below to complete the form correctly.
- Begin by downloading the DD 2870 form from the official website or obtaining a hard copy from the appropriate military office.
- Carefully read the instructions provided on the form to understand the requirements.
- In the first section, enter your personal information. This includes your full name, Social Security number, and contact details.
- Provide your military affiliation. Indicate whether you are active duty, a veteran, or a dependent.
- Fill in the section regarding the nature of your request. Be clear and concise about what you are seeking.
- In the next section, disclose any relevant information that may assist in processing your request. This could include dates, locations, or specific incidents.
- Review the certification statement carefully. By signing, you are affirming that all information provided is accurate and complete.
- Sign and date the form at the designated area. Ensure your signature matches the name provided at the top.
- Finally, submit the completed form according to the instructions provided. This may involve mailing it to a specific address or submitting it electronically.